


The Case for Rural Emergency Hospitals: The New REH is Access to Care
-
Category
Innovation -
Posted By
J.R. Robertson -
Posted On
Feb 09, 2023
Since 2012, rural hospital closures have accelerated due to factors including unfavorable reimbursements, ongoing operational costs, and declining and exceedingly sicker populations. These closures have resulted in underserved communities where residents may have to travel miles for access to emergency and other healthcare needs. Consequently, Congress launched the Consolidated Appropriations Act of 2021. This act created the new Rural Emergency Hospital (REH) designation available to existing rural hospitals with 50 or fewer beds, including Critical Access Hospitals. REH will provide emergent and outpatient care but will cease inpatient care.
Among other requirements, the final rule states that an REH must be enrolled in the Medicare program, provide 24/7 emergency department services with observation beds available, and, at the election of the REH, provide outpatient services. In some cases, hospitals may elect to convert inpatient beds to post-hospital extended care services provided under a licensed skilled nursing facility (SNF) designation. Hospitals that choose to participate in the REH program may do so as early as this month.
Given outpatient services have expanded while inpatient care has decreased in rural communities where bed capacity often exceeds need, this is a logical advancement. Rural or community hospitals that opt for this designation will receive a fixed monthly payment, plus a 5% add-on to the Medicare Outpatient Prospective Payment System (OPPS). Reimbursements are evaluated annually.
The REH must have a fully staffed emergency department, a physician, nurse practitioner, clinical nurse specialist, or physician assistant available to administer rural emergency hospital services in the facility. Certain patients will be treated or stabilized and transferred to regional medical centers as needed to treat high risk patients. Transfer agreements with regional tertiary care facilities will be activated. Provisions within the REH allow for outpatient specialists to rotate through on a scheduled basis. Finally, most, if not all outpatient procedures are permitted to be advanced, provided, and invoiced as being hospital-based.
So, what will a REH look like?
An REH program for design and construction will vary between communities. At a minimum, they will provide 24/7 emergency care. At the election of the community or the provider, they will build space for a variety of outpatient services. Existing facilities that elect to renovate may choose to convert inpatient beds to long-term skilled nursing or extended stay rehabilitation beds.
A baseline program for emergent care design will include at least one trauma in a segregated area and it should be adjacent to ambulance services. A decontamination and provisions for EMS; exam rooms suitable for pediatric and adult care should also be included. Some facilities may require isolation or negative pressure rooms. All should include space for a small observation unit. Although exam rooms can be utilized for minor procedures, a dedicated procedure room or two should also be programmed. The walk-in or public access area will include reception, waiting, and triage.
Outpatient services will vary by location, so flexibility should be considered. These exam rooms can be utilized for follow up visits for orthopedics, cardiac care, and endoscopy procedures when specialists rotate through. Other facilities might consider dialysis or oncology care in partnership with providers. Many facilities may include space for wellness or patient outreach programs.
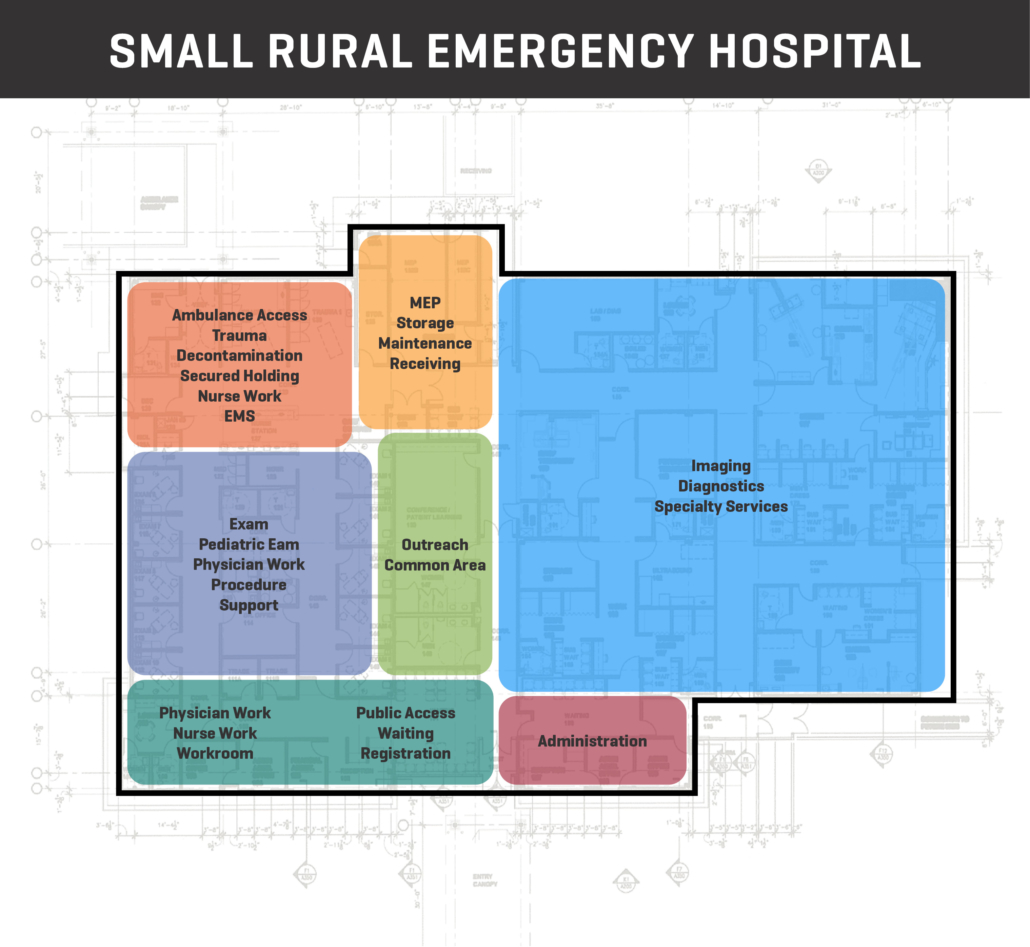
This baseline program for a small facility can be as small as 20,000 GSF. Site amenities would include adequate parking, a helipad, and flexible space for future expansion.
The block diagram below illustrates a potential program for an REH.
The REH enhances lives with convenient access to care. The REH also can be considered an important contributor to a town or region’s economic development efforts. Companies may consider access to care, when selecting a community for expansion. Likewise, companies also should consider access to this type of care for current or future employees.
While this new federal program is still evolving, we are confident that in time, we will learn more about how it will benefit underserved populations. Watch for future updates, and for more information on REH design, let’s talk.
Share this post on


